
You are now leaving the site
Are you sure you want to leave?
Are you sure you want to leave?

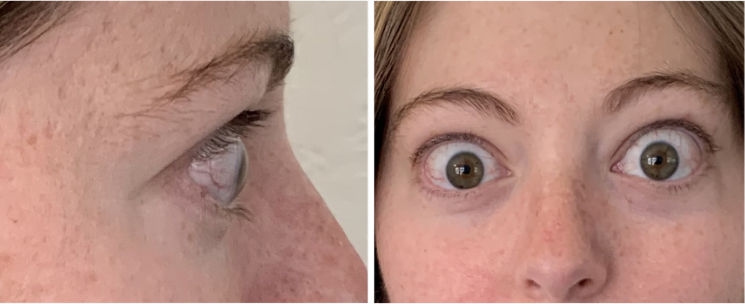
Visible signs:
Proptosis (28 mm OD; 25 mm OS), eyelid swelling, conjunctival redness
Nonvisible symptoms:
Intermittent diplopia
Impact on daily living:
Difficulty reading, lowered self-esteem
See the Burden-Impact Model for this patient
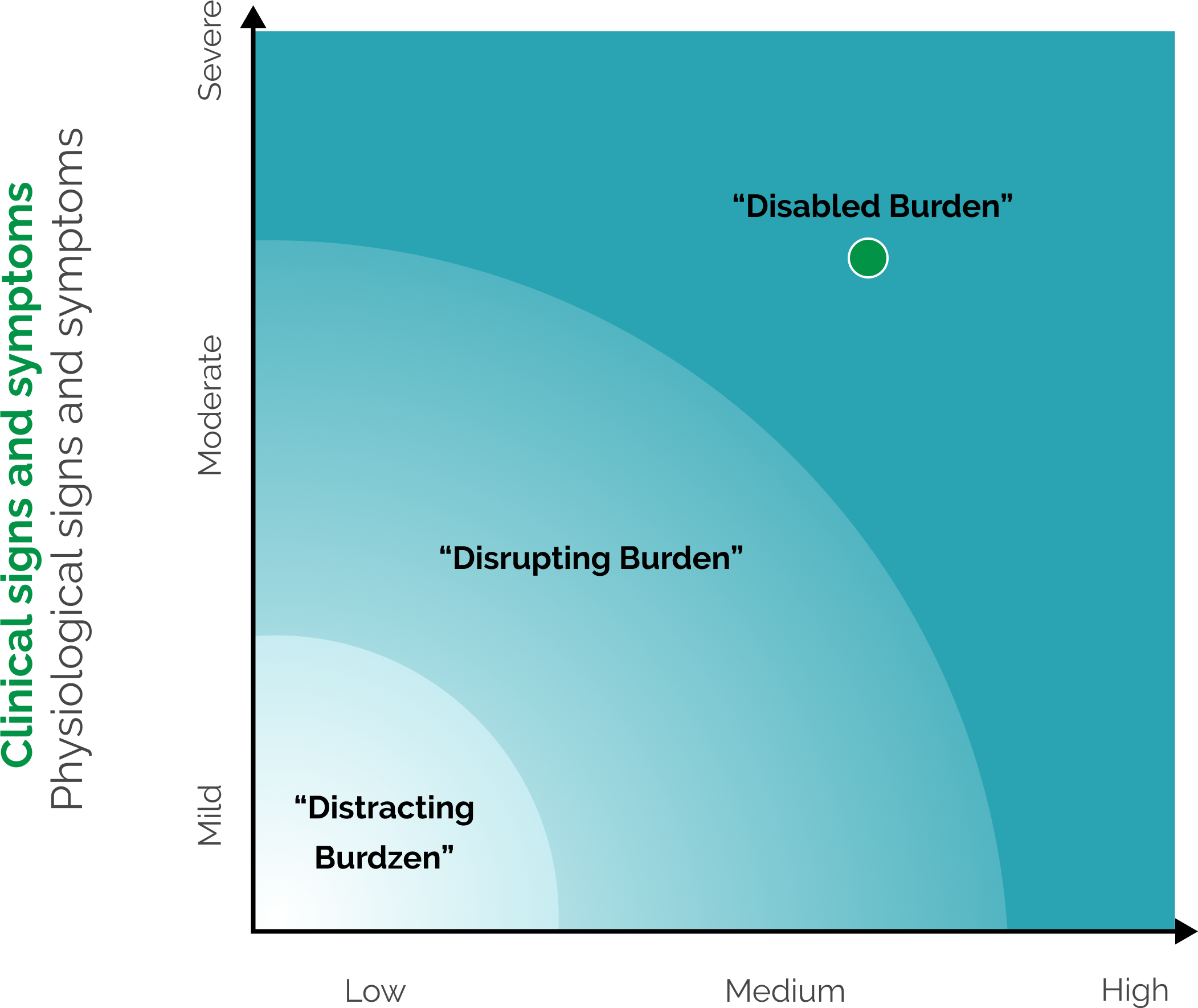
Patient-Reported Impact
Degree to which symptoms impact patients’ daily activities and emotional well-being
Not an official medical tool.

Some examples: eye pain, redness, swelling, eye bulging, and double vision. These are not all the signs and symptoms of TED


Some examples: walking outdoors, driving, reading


Some examples: negative impact to self-esteem, hiding their appearance in public


Visible signs:
Proptosis (24 mm OD; 22 mm OS)
Nonvisible symptoms:
Diplopia resolved
Daily living:
“I’ve been treating patients with TEPEZZA since 2020 and it has had a huge impact.” – Amina Malik, MD
See the Burden-Impact Model for this patient
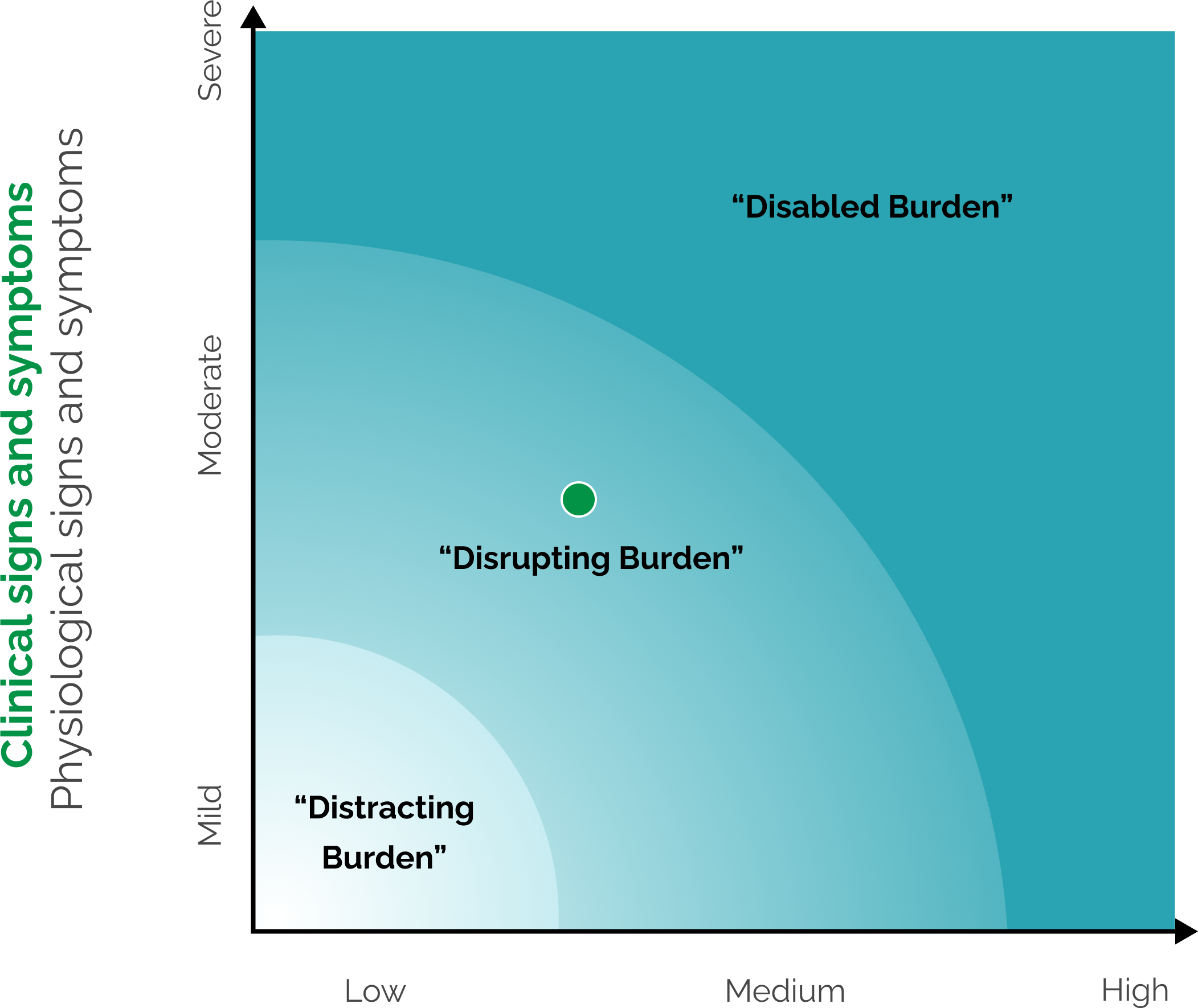
Patient-Reported Impact
Degree to which symptoms impact patients’ daily activities and emotional well-being
Not an official medical tool.
Signs and SYMPTOMS5,6
Some examples: eye pain, redness, swelling, eye bulging, and double vision. These are not all the signs and symptoms of TED

Daily Activities7,8
Some examples: walking outdoors, driving, reading

Emotional well-being9-10
Some examples: negative impact to self-esteem, hiding their appearance in public


Visible signs:
Proptosis (22 mm OD; 23 mm OS), eyelid swelling, conjunctival redness
Nonvisible symptoms:
Constant diplopia, eye pain, and burning sensation
Impact on daily living:
Lowered work productivity due to diplopia; reduced self-esteem
See the Burden-Impact Model for this patient
Patient-Reported Impact
Degree to which symptoms impact patients’ daily activities and emotional well-being
Not an official medical tool.
Some examples: eye pain, redness, swelling, eye bulging, and double vision. These are not all the signs and symptoms of TED
Some examples: walking outdoors, driving, reading
Some examples: negative impact to self-esteem, hiding their appearance in public

Visible signs:
Proptosis (20 mm OD; 21 mm OS)
Nonvisible symptoms:
Intermittent diplopia, eye pain and burning sensation resolved
Daily living:
Patient reported improvement in daily activities; happy with results
See the Burden-Impact Model for this patient
Patient-Reported Impact
Degree to which symptoms impact patients’ daily activities and emotional well-being
Not an official medical tool.
Some examples: eye pain, redness, swelling, eye bulging, and double vision. These are not all the signs and symptoms of TED
Some examples: walking outdoors, driving, reading
Some examples: negative impact to self-esteem, hiding their appearance in public
Because each patient responds differently to treatment, it is important that patients complete the full TEPEZZA treatment course of 8 IV infusions as studied in clinical trials1







A full course of treatment with TEPEZZA is 8 IV infusions—one every 3 weeks. In the Phase 3 study, improvement of proptosis as measured by mean change from baseline was observed as early as 6 weeks and continued to improve through Week 24.1
Cases of patients with TED and their individual experiences with TEPEZZA. Individual results may vary. Clinical presentations represent a range of patients with TED. Patients with prior surgery or orbital radiation treatment for TED, history of compressive optic neuropathy, and concomitant steroid use were excluded from clinical trials for TEPEZZA.2-4
IGF-1R, insulin-like growth factor-1 receptor; IV, intravenous; MRI, magnetic resonance imaging; OD, oculus dexter; OS, oculus sinister; TED, Thyroid Eye Disease.
Receive the latest news and updates about TEPEZZA
Receive the latest news and updates about TEPEZZA
WARNINGS AND PRECAUTIONS
Infusion Reactions: TEPEZZA may cause infusion reactions. Infusion reactions have been reported in approximately 4% of patients treated with TEPEZZA. Reported infusion reactions have usually been mild or moderate in severity. Signs and symptoms may include transient increases in blood pressure, feeling hot, tachycardia, dyspnea, headache, and muscular pain. Infusion reactions may occur during an infusion or within 1.5 hours after an infusion. In patients who experience an infusion reaction, consideration should be given to premedicating with an antihistamine, antipyretic, or corticosteroid and/or administering all subsequent infusions at a slower infusion rate.
Inflammatory Bowel Disease: TEPEZZA may cause an exacerbation of inflammatory bowel disease (IBD). IBD has been reported in some patients without a prior diagnosis of IBD. Monitor patients for signs and symptoms of IBD. If IBD exacerbation is suspected, discontinue use of TEPEZZA.
Hyperglycemia: Increased blood glucose or hyperglycemia may occur in patients treated with TEPEZZA. In clinical trials, 10% of patients (two-thirds of whom had preexisting diabetes or impaired glucose tolerance) experienced hyperglycemia. Hyperglycemic events should be controlled with medications for glycemic control, if necessary. Assess patients for elevated blood glucose and symptoms of hyperglycemia prior to infusion and continue to monitor while on treatment with TEPEZZA. Ensure patients with hyperglycemia or preexisting diabetes are under appropriate glycemic control before and while receiving TEPEZZA.
Hearing Impairment Including Hearing Loss: TEPEZZA may cause severe hearing impairment including hearing loss, which in some cases may be permanent. Assess patients’ hearing before, during, and after treatment with TEPEZZA and consider the benefit-risk of treatment with patients.
ADVERSE REACTIONS
The most common adverse reactions (incidence ≥5% and greater than placebo) are muscle spasm, nausea, alopecia, diarrhea, fatigue, hyperglycemia, hearing impairment, dysgeusia, headache, dry skin, ear discomfort, weight decreased, nail disorders, and menstrual disorders.
INDICATION
TEPEZZA is indicated for the treatment of Thyroid Eye Disease regardless of Thyroid Eye Disease activity or duration.
Please see Full Prescribing Information for more information.
1. TEPEZZA (teprotumumab-trbw) [prescribing information] Amgen. 2. Smith TJ, Kahaly GJ, Ezra DG, et al. Teprotumumab for thyroid-associated ophthalmopathy. N Engl J Med. 2017;376(18):1748-1761. 3. Douglas RS, Couch S, Wester ST, et al. Efficacy and safety of teprotumumab in patients with thyroid eye disease of long duration and low disease activity. J Clin Endocrinol Metab. 2024;109(1):25-35. 4. Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med. 2020;382(4):341-352. 5. Barrio-Barrio J, Sabater AL, Bonet-Farriol E, et al. Graves' ophthalmopathy: VISA versus EUGOGO classification, assessment, and management. J Ophthalmol. 2015:2015:249125. 6. Bothun ED, Scheurer RA, Harrison AR, et al. Update on thyroid eye disease and management. Clin Ophthalmol. 2009;3:543-551. 7. Cockerham KP, Padnick-Silver L, Stuertz N, et al. Quality of life in patients with chronic Thyroid Eye Disease in the United States. Ophthalmol Ther. 2021;10:975-987. 8. Park JJ, Sullivan TJ, Mortimer RH, et al. Assessing quality of life in Australian patients with Graves’ ophthalmopathy. Br J Ophthalmol. 2004 Jan;88(1):75-78. 9. Kahaly GJ, Petrak F, Hardt J, et al. Psychosocial morbidity of Graves' orbitopathy. Clin Endocrinol (Oxf). 2005:63(4):395-402. 10. Estcourt S, Vaidya B, Quinn A, et al. The impact of thyroid eye disease upon patients' wellbeing: a qualitative analysis. Clin Endocrinol (Oxf). 2008:68(4):635-639.

